Chronic Myeloid Leukaemia (CML)

Chronic Myeloid Leukaemia (CML), also known as Chronic Myelogenous Leukaemia, is a cancer of the blood and bone marrow. The term “chronic” indicates that this cancer grows more slowly than acute forms of leukaemia.
CML causes an overproduction of abnormal granulocytes (a type of white blood cell), crowding the bone marrow and preventing it from producing normal blood cells. This results in insufficient normal red blood cells, white blood cells and platelets circulating in the body.
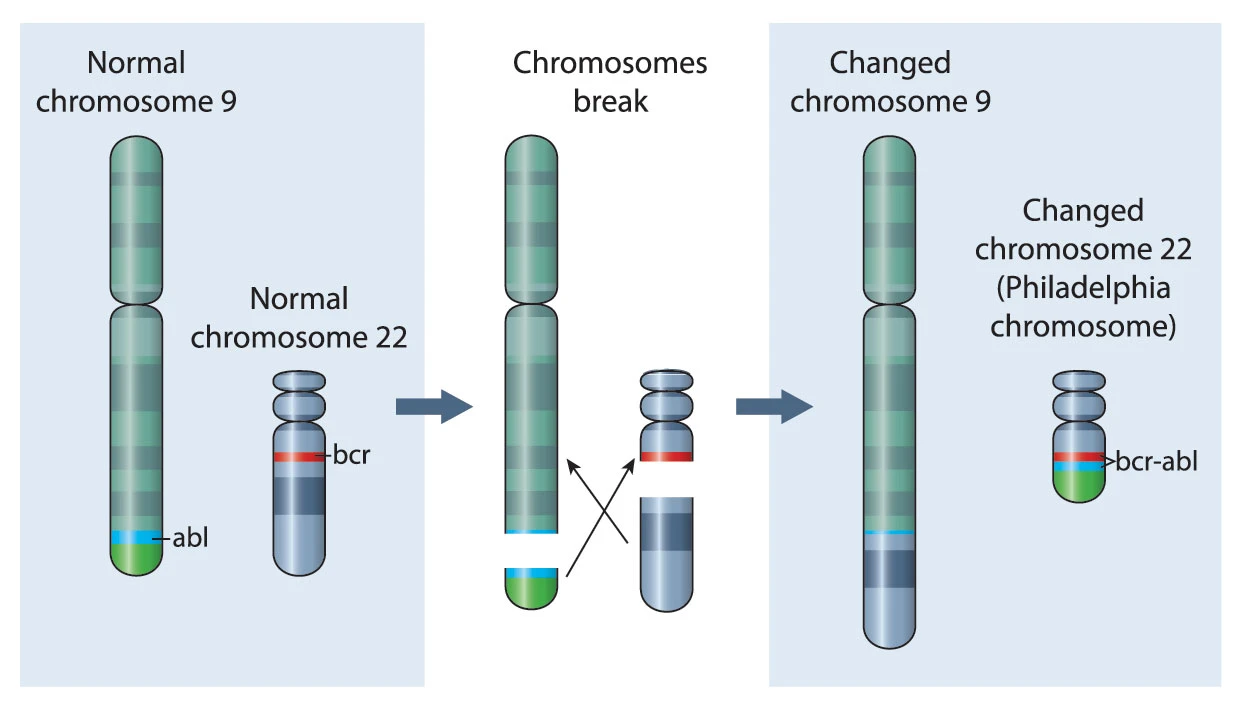
It has been found that most patients with CML have a gene mutation or abnormal chromosome called the Philadelphia chromosome. The Philadelphia chromosome is not hereditary, that is, it is not passed down from parent to child.
However, the exact cause of CML is not known. There are only a few risk factors for CML:
- Age – CML is more common in people over the age of 60. It is rare in children and teens.
- Gender – CML occurs slightly more frequently in men than in women.
- Exposure to radiation – Exposure to high doses of radiation (for example, from an atomic bomb blast or nuclear reactor accident) increases the risk of developing CML.
As CML usually grows slowly, it may take some time for symptoms to appear. CML may cause only mild symptoms and many people may not experience any symptoms at all. CML may even be discovered accidentally during a routine blood test. Common symptoms associated with CML are:
- Fatigue
- Fever
- Pale skin
- Breathlessness
- Weakness
- Loss of appetite
- Weight loss
- Night sweats or excessive sweating
- Bleeding gums or nosebleeds
- Bruising easily
- Bone pain
- Feeling of fullness in the stomach or swollen stomach
- Itching
- Frequent infections
If CML is suspected, a physical examination, blood test and bone marrow biopsy will help in giving a diagnosis.
In the physical examination, the doctor will check for signs of disease, such as swelling in the spleen.
The blood test, called a full blood count, involves a sample of blood being sent to the laboratory for investigation. The blood sample will be checked for the number of red blood cells, white blood cells and platelets. A high proportion of white blood cells may indicate CML.
A bone marrow biopsy involves taking a sample of bone marrow, usually from the hip bone. This is done under local anaesthetic and takes 15 – 20 minutes. The sample will also be sent for investigation by the aboratory, to be examined for cancerous cells.
Further tests, such as genetic testing and imaging tests (scans and ultrasounds), may be done to determine the extent of the CML and to help determine the best treatment options.
For most cancers, staging or determining the stage of cancer is helpful in deciding on treatment options. While most cancers are staged based on the size of the tumour and how far the cancer has spread in the body, the prognosis for CML depends on its phase as well as the amount of blasts (immature white blood cells) in the blood or bone marrow, among other factors.
CML is classified into three groups or phases. The cutoffs for the phases below were proposed by the World Health Organization (WHO):
- Chronic phase – Patients have less than 10% blasts in their blood or bone marrow samples. Symptoms are mild or absent. Most patients are diagnosed in this phase, and the phase can last for several years. Patients usually respond to standard treatments.
- Accelerated phase – Any of the following: Patients have 15% or more, but less than 30% blasts in their blood or bone marrow samples; 20% or more basophils (a special type of white blood cell) in the blood or bone marrow samples; blasts and promyelocytes together make up 30% or more of blood or bone marrow samples; platelet counts are very low (100 x 1,000/mm3 or less); thereare new chromosome changes in the leukaemia cells containing the Philadelphia chromosome. Patients may experience fever, weight loss or loss of appetite. Patients do not respond to standard treatments as well as in the chronic phase.
- Blast phase (or blast crisis) – Patients have 20% or more blasts in their blood or bone marrow samples. There are large clusters of blasts in the bone marrow, and blast cells have spread beyond the bone marrow. Patients may experience fever, weight loss and loss of appetite. This is the most aggressive stage of CML, and the symptoms are similar to those of Acute Myeloid Leukaemia (AML).
Treatment during the chronic phase may prevent CML from progressing to the more advanced phases. Some of the standard treatment options are targeted therapy, chemotherapy and immunotherapy. A stem cell transplant may also be offered to patients who do not respond well to targeted therapy.
Targeted Therapy
In targeted therapy, drugs or other substances target specific cancer cells to destroy or block their growth, while leaving normal cells unharmed. For CML, drugs called tyrosine kinase inhibitors or TKIs target the BCR-ABL tyrosine kinase enzyme and stop it from working, whichin turn causes the CML cells to die quickly. TKIs are often recommended as the first treatment for CML.
Chemotherapy
Chemotherapy is only used for more aggressive forms of CML nowadays, as targeted therapy is highly effective for the vast majority of cases of CML.
Chemotherapy uses drugs to destroy cancer cells or stop them from multiplying. The drugs may be given intravenously (through a vein in the hand or arm) or in tablet form. Two or more chemotherapy drugs may be combined. Chemotherapy is done in cycles with rest periods in between for the body to recover from the side effects of the drugs.

Immunotherapy
Immunotherapy involves using man-made or naturally produced substances to help the patient’s immune system to identify and destroy cancer cells. Interferon is a type of immunotherapy that works by lowering the number of white blood cells. It may also lower the number of cells containing the Philadelphia chromosome. Interferon is given via injections on a daily or weekly basis.
Stem Cell Transplant
A stem cell transplant may be done to replace bone marrow containing leukaemia with stem cells that develop into healthy bone marrow. This is considered an option only in patients who have advanced forms of CML.
The stem cells will need to come from a donor who is a close match to the patient, so the stem cells are not rejected by the patient’s body.
As there are very few known risk factors for CML, most of which cannot be avoided, there is no known way to prevent CML.
CanHOPE is a non-profit cancer counselling and support service provided by Parkway Cancer Centre, Singapore. CanHOPE consists of an experienced, knowledgeable and caring support team with access to comprehensive information on a wide range of topics in education and guidelines in cancer treatment.
CanHOPE provides:
- Up-to-date cancer information for patients including ways to prevent cancer, symptoms, risks, screening tests, diagnosis, current treatments and research available.
- Referrals to cancer-related services, such as screening and investigational facilities, treatment centres and appropriate specialist consultation.
- Cancer counselling and advice on strategies to manage side effects of treatments, coping with cancer, diet and nutrition.
- Emotional and psychosocial support to people with cancer and those who care for them.
- Support group activities, focusing on knowledge, skills and supportive activities to educate and create awareness for patients and caregivers.
- Resources for rehabilitative and supportive services.
- Palliative care services to improve quality of life of patients with advanced cancer.
The CanHOPE team will journey with patients to provide support and personalised care, as they strive to share a little hope with every person encountered.