Oesophageal Cancer
Overview
What is Oesophageal Cancer?
Oesophageal or Esophageal cancer is a disease in which malignant (cancerous) cells form in the inner lining of the oesophagus. The oesophagus is a muscular, hollow tube that runs from the throat to the stomach. Food is transported from the mouth to the stomach through the oesophagus to be digested.
Oesophageal cancer is often difficult to detect and is diagnosed late for several reasons:
The oesophagus is very flexible and can expand around the tumour as it grows. Hence, the early stages of oesophageal cancer tend not to show any signs or symptoms.
The signs of oesophageal cancer, when present, can be vague and similar to other more common abdominal conditions.
Types of Oesophageal Cancers
Oesophageal cancer is categorised based on the type of cell where the cancer originated from1,2:
Squamous cell carcinoma (also called epidermoid carcinoma): This cancer develops in the squamous cells that line the inner oesophagus and can occur anywhere along the oesophagus, but is most common in the upper and middle parts. Squamous cell carcinoma is the most common type of oesophageal cancer worldwide.
Adenocarcinoma: To develop adenocarcinoma of the oesophagus, squamous cells that normally line the oesophagus are replaced by gland cells. This typically happens in the lower oesophagus near the stomach and is largely due to persistent acid exposure in the lower oesophagus coming up from the stomach. It is more common in higher income countries where modern lifestyle choices have contributed to increased body weight.
Other rare types: Some rarer forms of oesophageal cancer that develop from other cells in the oesophagus include small cell carcinoma, sarcoma, lymphoma, melanoma and choriocarcinoma.
The majority of oesophageal cancers in Singapore are squamous cell carcinomas although the number of adenocarcinomas is gradually increasing.
How Common is Oesophageal Cancer?
Oesophageal cancer is the seventh most common cancer (3% of all cancer cases), and sixth leading cause of cancer deaths (6% of all cancer deaths) worldwide3. About 75% of all new cases and deaths from oesophageal cancer are reported in Asia, making it a significant health challenge in this part of the world4. However, it is relatively less common in Singapore, accounting for less than 1% of all cancer cases diagnosed here and less than 2% of cancer deaths5.
The incidence (number of cases) of oesophageal squamous cell carcinoma is in decline overall and this is thought to be attributable to economic gains and dietary improvements in developing countries, and a reduction in cigarette smoking in higher-income countries. The incidence of oesophageal adenocarcinoma, on the other hand, is rapidly rising particularly in wealthier Western countries, with excess body weight, gastroesophageal reflux disease and Barrett’s oesophagus among the key contributors (see Oesophageal Cancer Risk Factors below for more information)3.
Causes & Symptoms
What causes Oesophageal Cancer?
Oesophageal cancer begins when something triggers the cells in the inner lining of the oesophagus to develop mutations (changes) in their DNA that cause them to grow abnormally and develop into a tumour that can grow to invade nearby structures and spread to other parts of the body. The exact trigger for the mutation is not fully understood yet.
Oesophageal Cancer Risk Factors
There are certain risk factors that increase the chance of DNA damage in cells that may lead to oesophageal cancer. Some are more likely to increase the risk for squamous cell carcinoma and others for adenocarcinoma (See Types of Oesophageal Cancer for further detail).
Risk factors for oesophageal squamous cell carcinoma include6,7,8.9:
Smoking: Smoking cigarettes, cigars or a pipe, or chewing tobacco is a major risk for developing oesophageal squamous cell carcinoma. The longer you smoke, the higher the risk.
Betel Nut: Chewing betel nut (also known as areca nut) is a risk factor for squamous cell carcinoma especially in Asian countries. Those who indulge in both betel nut chewing and tobacco smoking are at even greater risk10.
Alcohol: The more alcohol someone consumes, the higher the likelihood of getting oesophageal cancer. In addition, smoking combined with alcohol intake raises the risk much more than either on its own6.
Diet: A diet low in fruits and vegetables increases the risk for squamous cell carcinoma. In addition, poor nutritional status is also a cause of oesophageal cancers particularly in developing nations.
Hot Beverages: Frequently drinking very hot liquids (temperatures of 65°C or more) may lead to long-term damage in the cells lining the oesophagus and increase the risk of squamous cell carcinoma.
Human papillomavirus (HPV): HPV is a common virus that can cause growths to develop on the vocal cords, mouth, hands, feet and genitals. Infection with certain types of HPV is linked to a number of cancers, including throat, oesophageal, anal and cervical cancers.
Underlying oesophageal diseases: Conditions that lead to structural changes in the oesophagus are associated with an increased risk of squamous cell carcinoma. Achalasia is a condition in which the muscle at the junction between the oesophagus and stomach (known as the lower oesophageal sphincter) does not relax properly, causing food and liquid to collect in the lower oesophagus. The cells lining the lower oesophagus can become damaged from being in contact with foods for longer than normal and may develop into cancer cells over time. Other causes of structural changes to the oesophagus include caustic strictures (scar tissue from ingestion of corrosive material) and gastrectomy (surgical removal of the whole or part of the stomach).
Hereditary conditions: Tylosis is a rare, inherited disease characterised by excessive growth of the top layer of skin on the palms of the hands and soles of the feet. People with this condition also develop small growths in the oesophagus and have a very high chance of getting squamous cell cancer of the oesophagus.
Risk factors for oesophageal adenocarcinoma include6,7,8.9:
Smoking: Someone who smokes a pack of cigarettes or more a day has at least twice the risk of getting oesophageal adenocarcinoma than a non-smoker, and the risk unfortunately does not reduce when the person stops smoking6.
Gastro-oesophageal reflux disease (GORD): GORD occurs when acid escapes from the stomach into the lower part of the oesophagus. People with GORD, especially those who have more frequent or long-standing symptoms have a higher likelihood of getting oesophageal adenocarcinoma6. However, GORD is a very common condition, and most people who have it do not develop oesophageal cancer.
Barrett’s oesophagus: This is a condition in which squamous cells lining the lower part of the oesophagus change into abnormal gland cells that resemble stomach or intestinal lining, usually as a result of persistent acid reflux. People with Barrett’s oesophagus are at a significantly greater risk of developing adenocarcinoma of the oesophagus, especially those who have more abnormal cells (high grade dysplasia) and longer parts of the oesophagus affected10.
Obesity: Being overweight (Body Mass Index, BMI of 25 to 30) or obese (BMI above 30) increases the probability of getting adenocarcinoma of the oesophagus. This is possibly due to the fact that people who carry excess body weight are more likely to have GORD.
Hereditary conditions: Peutz–Jeghers syndrome and Cowden syndrome are rare autosomal dominant conditions with increased risk of oesophageal cancer.
Having one or more of these risk factors does not automatically mean that you will get oesophageal cancer. Many people with risk factors never develop oesophageal cancer, whilst some with no known risk factors do.
What are the Signs and Symptoms of Oesophageal Cancer?
This cancer has few or no symptoms in the early stages, which makes early detection difficult. When they do occur, signs and symptoms of oesophageal cancer may include2,8:
- Difficulty or pain when swallowing
- Sensation of food stuck in the chest
- Choking on food
- Unintentional weight loss
- Indigestion and heartburn
- Burning pain in the chest, behind the breastbone
- Persistent coughing
- Hoarse voice
- Vomiting or coughing up blood
Most of these symptoms are more likely to be caused by common ailments such as acid reflux or a stomach ulcer. However, if you have any of these symptoms, especially if they persist or get worse, you should see a doctor to have it checked out and treated if needed.
Diagnosis & Assessment
Diagnosis of Oesophageal Cancer
If you have symptoms or signs that suggest oesophageal cancer, your doctor will investigate further to determine if you have cancer. Oesophageal cancer can be detected through the following procedures and tests1,11:
Clinical history and examination: Your doctor will ask about your personal and family medical history and perform a physical examination of your abdomen.
Blood tests: Blood tests to check your general health including your kidney and liver function will be done.
Endoscopy: During this procedure, the doctor puts an endoscope (a long flexible tube with a camera and light at the end) into the mouth and down into the oesophagus. A biopsy (tissue sample) may be taken using instruments inserted through the endoscope if any abnormal areas are seen.
Barium swallow x-ray: This test involves swallowing a liquid contrast (barium) to coat the inner lining of the oesophagus followed by x-ray imaging. It is used less often than endoscopy to look for oesophageal cancer, as it can miss some abnormal areas, and it cannot take biopsy samples. But it is less invasive than endoscopy and may be useful in certain situations.
Biopsy sample testing: Samples of cancer cells obtained through biopsy is tested in the laboratory to provide further information on the type of oesophageal cancer it is. In addition, biomarker testing may be done to look for specific genes, proteins and other substances (called biomarkers or tumour markers) that the cancer cells might have. The presence of biomarkers can guide cancer treatment selection.
How is Oesophageal Cancer Assessed?
After oesophageal cancer has been diagnosed, your doctor will determine the extent (stage) of the disease. Staging may be done using the following tests11:
Imaging tests: Computed tomography (CT) scans and/or positron emission tomography-CT (PET-CT) scans of the chest and abdomen are done to look for evidence of distant cancer spread to other organs such as the liver and lungs.
Endoscopic ultrasound (EUS): EUS is the standard test for locoregional staging, which is the assessment of tumour depth (how far the cancer has grown into the oesophageal wall) and spread to local region (lymph nodes or tissues near the oesophagus). An endoscope with an ultrasound tool is inserted down the throat and into the oesophagus to generate pictures of the oesophagus, nearby organs and lymph nodes. A biopsy of any suspicious areas may also be done under ultrasound guidance.
Bronchoscopy: This endoscopic test may be done in cases where the cancer is in the upper part of the oesophagus to see if it has spread to the trachea (windpipe) or the bronchi (tubes leading from the windpipe into the lungs).
Laparoscopy: This procedure may be done for some patients with locally advanced adenocarcinoma of the oesophagus who may have small metastasis (spread) that may have been missed on CT or PET-CT (also known as occult metastasis). During this surgical procedure, a few small incisions (cuts) is made in the abdomen and an endoscope is inserted. This allows the surgeon to view the space around the abdomen to look for abnormalities or signs of cancer spread.
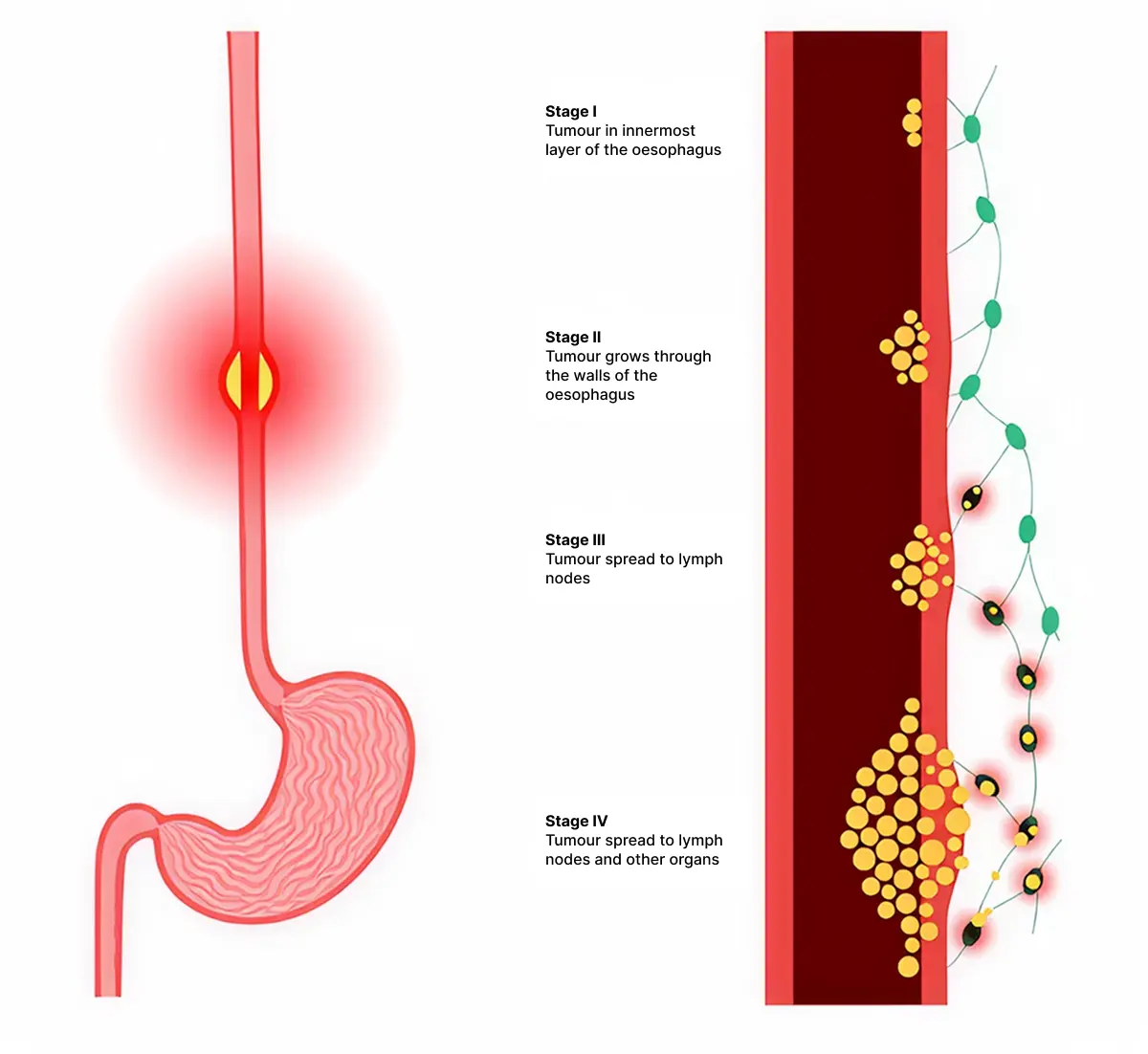
Doctors describe oesophageal cancer stages as12,13:
Stage 0: Abnormal cells (not yet cancer) are found only in the inner lining of the oesophagus. Stage 0 is also called high-grade dysplasia.
Stage I: Cancer cells are found only in the layer of cells that line the oesophagus.
Stage II: The cancer has reached the muscle layer or the outer wall of the oesophagus. In addition, the cancer may have spread to 1 to 2 nearby lymph nodes.
Stage III: The cancer has directly invaded into the lymph nodes adjacent (next to) the oesophagus.
Stage IV: The cancer has directly invaded into the deepest muscle layer of the oesophagus and/or spread to other organs in the body such as the lungs, liver, distant lymph nodes, and bones.
Treatment of Oesophageal Cancer
Oesophageal Cancer Treatment Options
When considering your treatment plan your doctor will take into account the following factors9:
- The stage of your cancer when it is discovered.
- The location of the tumour.
- Your overall health and nutrition levels.
- Your preferences.
The first goal of oesophageal cancer treatment is to get rid of the cancer. When that is unachievable, the focus may be on stabilising the cancer to prevent its progression for as long as possible and improving quality of life. Oesophageal cancer can be treated with the following methods, often used in combination2,7,8:
Surgery: Very early-stage oesophageal cancer can often be treated and possibly cured with surgery. Unfortunately, most oesophageal cancers are not found early enough for this to happen. In most cases, additional treatment before surgery (known as neoadjuvant therapy) or after surgery (known as adjuvant therapy) is usually recommended. This may involve chemotherapy and radiotherapy. Surgical procedures used to treat oesophageal cancer include:
Endoscopic mucosal resection: Very small stage 0 or stage I cancers can be cut away from the inside lining of the oesophagus. To remove the cancer, an endoscope is passed down the throat and into the oesophagus. Special cutting tools are passed through the scope to cut out the cancer with a margin of healthy tissue.
Oesophagectomy: During oesophagectomy, the surgeon removes the part of the oesophagus that contains the cancer and some nearby lymph nodes. Sometimes, the upper part of the stomach may need to be removed as well. The remaining section of the oesophagus is then reattached to the stomach to re-establish the digestive tract. Surgery is usually done as a minimally invasive procedure, where special surgical tools are inserted through several small incisions.
Chemotherapy: Chemotherapy is the use of drugs to kill cancer cells or stop them from dividing. The drugs enter the bloodstream and can affect cancer cells all over the body. Giving chemotherapy before surgery to shrink the cancer for easier removal is called neoadjuvant chemotherapy. Chemotherapy might also be used after surgery if there is a risk that some cancer cells have been left behind. Giving chemotherapy after surgery is called adjuvant chemotherapy. It can be given alone or in combination with radiotherapy. Chemotherapy may also be used to relieve symptoms or prolong life in patients with advanced stomach cancer that cannot be operated upon.
Radiation therapy (Radiotherapy): Radiotherapy uses powerful, high-energy beams to kill cancer cells. It can be used either before surgery to shrink the size of the tumour or after surgery to destroy any remaining cancer cells, and is commonly combined with chemotherapy. Patients who are unable to have surgery due to poor general health may be treated with radiotherapy combined with chemotherapy as the main treatment. In patients with advanced oesophageal cancer, radiotherapy may be useful for relieving oesophageal obstruction (blockage), reducing pain and stopping bleeding from cancers that cannot be operated on. There are various radiotherapy options including proton therapy that may result in less long-term side effects.
Targeted therapy: Targeted therapies are drugs that block the growth and spread of cancer by interfering with specific molecules involved in tumour growth and spread. Monoclonal antibodies are a form of treatment that target specific proteins on oesophageal cancer cells, such as HER2 and VEGF, to stop the cells from growing. Targeted therapy may be combined with chemotherapy for advanced oesophageal cancers that cannot be surgically removed or for cancers that recur after treatment.
Immunotherapy: Immunotherapy uses the body's natural defences to fight cancer by enhancing the immune system's ability to attack cancer cells. In recent years, immunotherapy drugs called immune checkpoint inhibitors, PD-1 inhibitors and CTLA-4 inhibitors have been approved as adjunct (additional) therapy and to treat advanced oesophageal cancer that cannot be removed by surgery or have come back after treatment.
Supportive (palliative) therapy: Supportive therapy is treatment aimed at relieving symptoms to improve quality of life instead of trying to cure the cancer. The following procedures are often carried out to address common symptoms experienced by oesophageal cancer patients, especially those with advanced stage disease:
Oesophageal dilatation: This procedure is used to expand an area of the oesophagus that is narrowed or blocked in order to improve swallowing. This can be done by placing a stent (a thin wired tube) through the tumour to hold the oesophagus open, or using laser or heat sources to break down the cancer.
Feeding tube insertion: Oesophageal cancer can cause problems with swallowing making it hard to maintain good nutrition, and together with the general effects of the cancer, can lead to significant weight loss. Some people with oesophageal cancer may need to have a feeding tube (jejunostomy) which is inserted through the skin into the small intestine during a minor procedure. Liquid feeds can then be delivered directly into the small intestine to provide the required amounts of nutrition and calories.
Oesophageal Cancer Survival Rate
The outlook for oesophageal cancer is unfortunately poor at present, as most cases are in the advanced stages by the time they are diagnosed. The overall five-year survival rate is 22%. The best outcome is seen in those who are diagnosed in the very early stages, when the tumour is still confined to the oesophagus and can be removed completely with surgery. Unfortunately, only 25% of people with oesophageal cancers are diagnosed early enough for this to happen8. At later stages, oesophageal cancer can still be treated but rarely cured15.
It is worth noting that survival rates are grouped based on stage (how far the cancer has spread), but other factors such as your age, overall health and how well the cancer responds to treatment can also affect your prognosis (outcome). Even taking these things into account, the prognosis your doctor gives you will be an estimate based on the statistics we have of people who have had the same diagnosis. Your journey may still differ from another person’s in a similar situation.
Furthermore, breakthroughs in cancer research are happening at a faster pace than ever before, providing greater insights and leading to the development of more effective treatment options. Researchers are working hard to find novel ways to improve the outcome and quality of life for those diagnosed with oesophageal cancer. You may wish to speak to your treating doctor to find out if there are clinical trials suited to your individual situation.
Prevention & Screening
Oesophageal Cancer Screening
Screening refers to looking for cancer before a person has any symptoms. There is currently no recommended routine screening for oesophageal cancer for the general population. It is therefore important, especially if you have one or more risk factors (see Oesophageal Cancer Risk Factors above) to be vigilant and see your doctor for prompt investigation if you have any symptoms.
People at high risk of getting oesophageal cancer, such as those with Barrett’s oesophagus or inherited conditions like tylosis should be closely monitored, usually with regular endoscopy and biopsy of any abnormal areas seen. This may detect oesophageal cancer at an earlier stage when the cancer is localised and more easily removed by surgery. Those with Barrett’s oesophagus affecting a large area, or high-grade dysplasia may be advised to undergo treatment due to the high chance of adenocarcinoma developing (or already present)16.
Oesophageal Cancer Prevention
While there is no guaranteed way to prevent oesophageal cancer, there are some measures you can take to reduce your risk2,17:
Avoid or quit smoking: Smoking increases your risk of oesophageal cancer and many other types of cancers. Quitting smoking can be very hard, so ask your health care provider for help. These might include support groups, medicines and nicotine replacement therapy.
Limit or avoid alcohol consumption: Drink alcohol in moderation, if at all. For healthy adults, that means up to one drink a day for women of all ages and men older than 65 years, and up to two drinks a day for men aged 65 and younger.
Eat a healthy, balanced diet: A diet with less fat, sugar, red meat and processed foods, and more fresh fruits, vegetables and whole grains can help to reduce the risk of many diseases and cancers including oesophageal cancer.
Maintain a healthy body weight: A healthy diet and regular exercise can help you to keep to a healthy body weight and reduce your risk for many conditions including oesophageal cancer. If you are overweight or obese, talk to your doctor about strategies to help you lose weight in a safe manner.
Seek treatment for gastro-oesophageal reflux disease (GORD): Treating reflux may help prevent Barrett’s oesophagus and oesophageal cancer. Often, this is done with changes in diet and lifestyle (for example, weight loss for overweight individuals), as well as medications called H2 blockers or proton pump inhibitors (PPIs).
Frequently Asked Questions (FAQ)
The 5-year survival rate for someone with oesophageal cancer is around 22%14. This means that 22 out of 100 people with oesophageal cancer are alive five years after their diagnosis. This is largely due to the fact that most oesophageal cancers do not show symptoms until they have progressed to an advanced stage. If diagnosed and treated early (Stage 1), the 5-year survival rate can be up to 65%18.
It is important to understand that these statistical numbers are obtained from a group of people with the same diagnosis to represent an average. Individuals may differ in their own experience. It is best to discuss your prognosis (outcome) with your treating doctor who would be able to provide you with more specific information based on your personal circumstances.
It is often difficult to detect oesophageal cancer early because signs and symptoms usually do not appear until it has progressed to an advanced stage. There is currently no recommended screening tests available for the general population.
If you are at high risk for oesophageal cancer, for example if you have Barrett’s oesophagus, regular endoscopic surveillance is recommended to detect early cancerous changes (See Oesophageal Cancer Screening above).
Occasional acid reflux will not cause oesophageal cancer. However, repeated acid exposure over an extended period of time as seen in gastro-oesophageal reflux disease (GORD) may cause damage to the oesophagus and trigger changes in the cells in the inner lining of the oesophagus. In some cases, it can develop into Barrett's oesophagus which may progress to oesophageal adenocarcinoma down the track. However, it is worth nothing that whilst GORD is a common condition, most people with GORD do not end up having Barrett’s oesophagus or cancer.
In general, stage 0, I, and II and some stage III oesophageal cancers are potentially curable with surgery13. Unfortunately, whilst the cancer itself might be resectable (removable by surgery) many patients may not be suitable candidates for surgery due to poor health condition. The 5-year survival rate for those with oesophageal cancer that has not yet spread is close to 50%13.
Oesophageal cancer and its treatments can cause difficulties with swallowing and make it hard to eat well. It is important to eat and drink enough calories and nutrients to maintain your weight, strength and overall health.
You might find making certain changes to your diet helpful, such as:
Avoiding nutrient-poor foods: Where possible, choose healthy, nutrient-dense food options instead of empty calories/nutrient-poor foods such as sugary drinks, packaged snacks and carbohydrate-based desserts.
Avoiding foods that cause indigestion: Foods such as fizzy drinks, alcohol, spicy food, pickles, citrus fruits and caffeine can cause indigestion.
Avoiding foods that are hard to swallow or likely to stick in the throat: If you have difficulty swallowing, avoid raw hard fruits and vegetables, tough cuts of meat, soft doughy bread and very dry foods.
Having a healthy and balanced diet: A balanced diet with more fruits, vegetables and whole grains, and less preserved food, red meat and processed meats reduces the risk for many cancers and diseases.
If your stomach was used to replace part of the oesophagus following surgery to remove the cancer, the stomach might not be able to hold food for digestion as it did before, causing food to pass quickly into the intestine. This leads to a condition known as dumping syndrome which causes symptoms such as nausea, vomiting, diarrhoea, stomach cramps, sweating and flushing of the skin after eating. You may need to modify the way you eat19:
Eat smaller meals more frequently: Try having six smaller meals a day instead of three large meals.
Avoid sweets, simple carbohydrates and dairy: These foods tend to cause rapid blood sugar shifts. Choose complex carbohydrates such as whole grains instead.
Eat more protein and healthy fats: These slow down digestion and provide a steadier form of energy.
Eat more fibre: Dietary fibre adds bulk and helps to slow down movement of the food through the digestive tract.
Lie down on your back for 30 minutes after eating: This may slow down the emptying of food from the stomach into the intestine and help to maintain blood pressure during digestion.
Avoid fluids for 30 minutes before and after eating: This may help to slow down stomach emptying.
A dietician will be able to provide you with specific recommendations if you would like more support in this area. Speak to your doctor about a referral to a dietician with an interest in cancer care. Some patients may benefit from having a feeding tube put in temporarily to boost nutrition.
References
- WebMD. Esophageal Cancer: Everything You Need to Know. Accessed at https://www.webmd.com/cancer/esophageal-cancer on 19 July 2024.
- Mayo Clinic. Esophageal Cancer. Accessed at https://www.mayoclinic.org/diseases-conditions/esophageal-cancer/symptoms-causes/syc-20356084 on 19 July 2024.
- Sung H, Siegel RL, Laversanne M, et al. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA: A Cancer Journal for Clinicians 2021; 71(3):209-49.
- The Global Cancer Observatory, International Agency for Research on Cancer, World Health Organization. Oesophagus Fact Sheet. Accessed at https://gco.iarc.who.int/media/globocan/factsheets/cancers/6-oesophagus-fact-sheet.pdf on 19 July 2024.
- The Global Cancer Observatory, International Agency for Research on Cancer, World Health Organization. Singapore Fact Sheet. Accessed at https://gco.iarc.fr/today/data/factsheets/populations/702-singapore-fact-sheets.pdf on 19 July 2024.
- American Cancer Society. Esophageal Cancer Risk Factors. Accessed at https://www.cancer.org/cancer/types/esophagus-cancer/causes-risks-prevention/risk-factors.html on 19 July 2024.
- Mukkamalla SKR, Wang Y, Lyons S, et al. Esophageal Cancer. In: StatPearls [Internet]. Accessed at https://www.ncbi.nlm.nih.gov/books/NBK459267/ on 19 July 2024.
- Cleveland Clinic. Esophageal Cancer. Accessed at https://my.clevelandclinic.org/health/diseases/6137-esophageal-cancer on 19 July 2024.
- Johns Hopkins Medicine. Esophageal Cancer. Accessed at https://www.hopkinsmedicine.org/health/conditions-and-diseases/esophageal-cancer on 19 July 2024.
- Cancer Research UK. Risks and Causes of Oesophageal Cancer. Accessed at https://www.cancerresearchuk.org/about-cancer/oesophageal-cancer/causes-risks on 19 July 2024.
- American Cancer Society. Tests for Oesophageal Cancer. Accessed at https://www.cancer.org/cancer/types/esophagus-cancer/detection-diagnosis-staging/how-diagnosed.html on 19 July 2024.
- Cancer Research UK. Stages, Types and Grades of Oesophageal Cancer? Accessed at https://www.cancerresearchuk.org/about-cancer/oesophageal-cancer/stages-types-and-gradesr on 19 July 2024.
- American Cancer Society. Esophageal Cancer Stages. Accessed at https://www.cancer.org/cancer/types/esophagus-cancer/detection-diagnosis-staging/staging.html on 19 July 2024.
- American Cancer Society. Survival Rates for Esophageal Cancer. Accessed at https://www.cancer.org/cancer/types/esophagus-cancer/detection-diagnosis-staging/survival-rates.html on 19 July 2024.
- National Cancer Institute. Esophageal Cancer Treatment (PDQ®)–Patient Version. Accessed at https://www.cancer.gov/types/esophageal/patient/esophageal-treatment-pdq on 19 July 2024.
- American Cancer Society. Can Esophageal Cancer Be Found Early? Accessed at https://www.cancer.org/cancer/types/esophagus-cancer/detection-diagnosis-staging/detection.html on 19 July 2024.
- American Cancer Society. Can Esophageal Cancer Be Prevented? Accessed at https://www.cancer.org/cancer/types/esophagus-cancer/causes-risks-prevention/prevention.html on 19 July 2024.
- Cancer Research UK. Survival for Oesophageal Cancer. Accessed at https://www.cancerresearchuk.org/about-cancer/oesophageal-cancer/survival on 19 July 2024.
- Cleveland Clinic. Dumping Syndrome. Accessed at https://my.clevelandclinic.org/health/diseases/17835-dumping-syndrome on 19 July 2024.